
Applying Risk Theory to Occupational Health

I first came across James Reason’s (1990) Defence in Depth accident trajectory model, or as it is more commonly known the ‘Swiss Cheese model’, 12 years ago and it surprised me that this approach had not been adopted more widely in the area of occupational health.
Put simply, the Defence in Depth model (Figure 1) when used in an occupational health setting allows any organisation to build in layers of defence to safeguard against failure. Failure in this context can mean notifiable injuries, a loss in productivity due to ill health or post-employment claims.
What Reason proposes is that risk has a trajectory, which passes through corresponding holes in the layers of defence, barriers and safeguards and if it achieves a ‘direct flow through’, will result in a failure. Reason indicates that a Defence in Depth approach acknowledges that all systems are fallible and that by lining up layers of defence in depth, organisations are presented with the opportunity of catching, retarding or retiring risk prior to failure.
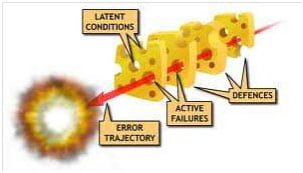
Figure 1: Defence in Depth Model (Reason, 1990)
Human risk factors essentially follow a similar trajectory in that there are both active failures and latent conditions (over a period of time combined with degenerative conditions) that coexist within the workplace and when these factors come together they often lead to poor health and result in poor productivity outcomes.
To apply the Defence in Depth theory in an occupational health setting, we will explore four critical health defence layers that can improve the ability to control health risks:
- Pre-Employment health screening
- Health Management (including health surveillance & assessments, wellbeing & absenteeism)
- Injury Management / Rehabilitation (Workers Compensation)
- Exit medicals
Each of these four key defence layers has the ability to “catch, retard or retire risk” so that an error trajectory is not achieved and more importantly, the likelihood of a failure is reduced significantly.
So, what are some of the challenges in applying the theory?
For many organisations the four critical health layers tend to be managed by separate departments and as such the information tends to remain in its “silo” and not used in a holistic view for improving health. This results in the organisation having little opportunity to prevent a direct flow through to a failure in health, as the data and learning’s from each area are often not available.
By way of example, we will consider the role that pre-employment screening has on other areas such as workers compensation claims.
Essentially, a pre-employment medical is used to help an organisation in the recruitment process increase the likelihood of hiring candidates that meet the inherent job requirements at an acceptable level of health risk both to the worker and the organisation. Every organisation accepts a certain level of risk when engaging and retaining employees. This risk is counterbalanced by reward for the organisation in measurable factors such as improved productivity.
By hiring the wrong worker in the wrong occupation, the organisation imports significant health risk directly into the business and may fail to realise any productivity gain and expose itself to workers compensation claims, increased absenteeism and adversely impact on the productivity of existing personnel (such as those engaged in human resources, training and line management).
A review of relevant and current literature indicates that non-screened employees have a 33% higher injury rate than screened employees, and the cost associated with these injuries is 4.3 times higher (Roshenblum & Shankar, 2006). The primary question to ask then appears to be: why is this type of information not used in a workers compensation setting?
A critical consideration is privacy. However, if the data is aggregated and used to identify common trends, privacy can be maintained and improvement actions put in place.
How could Defence in Depth be applied to occupational health?
In many industries a number of health defence layers already exist. Examples of these include preemployment medicals, periodic medicals, health surveillance activities, health risk assessments, wellbeing programs, flu vaccinations, EAP (Employee Assistance Programs) and exit medicals. Whilst they may exist in different combinations, a common challenge is that they tend not to form part of an overall health risk management strategy.
Lining all of the health components up and having a conduit between them becomes the key to releasing valuable, risk-based information that can greatly enhance any organisation’s ability to identify health risk trends, and then use this information in a positive way to reduce the likelihood of poor health outcomes, and deliver measurable business and employee benefits.
One of the best analogies I have come across for this was from a colleague who, in quite a candid manner, responded to this theory adaption by saying that this is really the same as an asset management system applied to our most important asset, people! And you know what, he was absolutely correct. Could you imagine an Asset Manager in a large organisation purchasing 200 new pieces of machinery and then just saying “go for it” to the workforce? “Just use them, and we won’t worry about any maintenance periods, pre-start checks, inventory control or systems to maintain them in a sound working order." Ironically, in many ways, this is exactly what we do with a workforce.
By applying the Defence in Depth approach to occupational health we would deliver the same level of control to productivity as we do to overall equipment efficiency, we would have a demonstrable way of valuing our most important asset and we could measure the financial benefits. To test this hypothesis further, let’s return to our previous example. Worker’s compensation data is usually only available within the claims and insurance area of a business and yet, this data can provide significant insight to pre-employment screening by identifying where the health risks reside.
Furthermore, insurance data can usually reveal which occupations are most likely to incur a workers compensation claim, at which sites and which activity (mechanism and injury location) was involved. At a pre-employment level, this information should be used to manage the health risks entering the business (targeted pre-employment medicals) and then should be further monitored to ensure that workers engaged in these higher risk roles have the appropriate health interventions and health surveillance activities implemented.
The key here is putting in place systems to protect our people and by interlinking these four health defence layers, even in a modularised approach, it affords a far greater ability to drill down into data and design health interventions based upon the actual identified health risks.
A good example to illustrate this point, in an industrial setting, is a dump truck driver on a mine site. Historically, these roles are undertaken on a rotating roster basis incorporating both day and night shifts on typically a 4-on/4-off roster or 7-on/7-off roster. This can be further complicated by a FIFO (Fly In - Fly Out arrangement) where there is little time afforded for healthy activities. Personal visits to numerous mine sites reveal there is a level of healthy eating programs instilled at an organisational level, however the lifestyle afforded to the workers engaged in these roles leaves them vulnerable to over period of time injuries such as back and neck and chronic health diseases.
These are now more commonly termed as lifestyle diseases such as obesity, nutritional diseases, high cholesterol, high blood pressure and diabetes. Most of the characteristics outlined above, if not managed properly, will lead to poor outcomes for the organisation in absenteeism, workers compensation claims and an overall loss to productivity. For the individual, these effects can be long term and ultimately affect their ability to engage in purposeful, productive work until retirement age. All of these factors merge together and are responsible for high disability adjusted life years. Using the dump truck driver example, most organisations engaged with these roles will have historical workers compensation experiences that will clearly point to both a ‘mechanism of injury’ and an ‘injury location’, which are in more cases than not, completely controllable.
At a pre-employment level, this workers compensation data needs to be analysed and the engagement medical modified to capture the risk factors, particularly around the neck and back (and any other types of injuries connected with the claims experience). From an individual perspective, this information can be used to monitor how the individual comes into the business and further, what health programs and interventions are put in place to manage them in the workplace. If a particular occupation shows trending in one type of injury, why would an organisation not put in a layered intervention (Defence in Depth) to retard or reduce both the likelihood and the impact of an injury occurring? This can be done through health promotions such as back care programs or periodic health reviews with ‘at risk’ workers to see if there has been any degradation or indeed improvement. When a worker leaves an organisation, there always remains the future possibility of an insurance claim for injuries sustained in the originating workplace, which have deteriorated over time. Most organisations play a form of ‘Russian roulette’ with exiting workers as there is more often than not, a complete inability to ascertain what level of risk they may present in the future.
The ‘dump truck driver working on a mine-site’ example illustrates the benefits of implementing a Defence in Depth strategy to occupational health. By aligning the four critical health defence layers (pre-employment, health management, injury/claims management and exit medical) within an organisation, the short term benefits will be achieved through a healthy, productive workforce that has dedicated health platforms in place to manage all ongoing health issues. The long term benefits will include a reduction and severity in workers compensation claims for existing employees, reduction in absenteeism and being able to impart a level of control to any future 3rd party claims for past employees who submit over period of time claims.
A Defence in Depth approach to health will, in my opinion, provide significant cost reductions to current siloed practices and lead to far greater measureable outcomes aimed at maintaining a fit and healthy workforce.
Mark Cassidy is GM of Risk and Innovation at 2CRisk. If you would like to find out more about how 2CRisk can help you tackle the challenges of health management, go to www.2CRisk.com.au or you can contact Mark on +61 1300 736 361 or e-mail info@2CRisk.com.au
James Reason (1990) Human Error, Cambridge University Press.
Published 15 September, 2012 | Updated 19 January, 2016